Digital Experience Design & Strategy
Designing a global UX framework that scales across markets, respecting cultural, regulatory, and health literacy differences while maintaining experience design consistency.
The experience design brief was built around a named patient persona (Andrea) with a documented emotional profile: frustrated, stuck, cycling through the same failed attempts, carrying both external and internal stigma, worried about her future health. Her experience was the design constraint. Everything from the homepage module sequence to the quiz learning prompt architecture was calibrated to resolve the specific emotional barriers Andrea carried before asking her to take any clinical action.
My role: I led global UX strategy and experience design — defining the IA, content hierarchy, and UX framework that coordinates across markets. I owned the global-to-local experience design logic and the dependency workflows between Lilly regional delivery teams.
Led agency-side, coordinating across UX, strategy, and global delivery before aligning with Lilly's global platform owners and four regional teams. Global principles had to be locked before regional teams could move. Governance logic was agreed across both organizations upfront — local adaptation proceeded without escalation.
A global platform request concealed two distinct structural problems that needed to be solved sequentially.
"Design a global obesity platform that can be adapted for each market — KSA, UAE, Germany, Japan — while maintaining brand and regulatory consistency."
The brief frames this as an adaptation problem. It's actually two problems: first, identify which UX elements are structurally non-negotiable globally and which are genuinely flex zones — and that distinction hasn't been made yet. Second, obesity is one of the most stigma-loaded health conditions globally, and the UX must address the emotional reality of a patient who likely carries years of failed interventions and self-blame before it can make any clinical ask. The platform design challenge is global architecture plus stigma-aware emotional sequencing, not localization of a standard pharma UX template.
This reframe produced the global/flex zone architecture — defining non-negotiables centrally while building structured local adaptation into specific modules — and drove the stigma-reduction UX sequencing that opened the homepage experience.
Global wellness platforms & stigma-adjacent health conditions. The global constants / local flex zones architecture applies to any health platform scaling across markets where a condition carries cultural stigma. The stigma-reduction sequencing transfers directly to weight management, mental health, addiction support, and any condition where self-blame is a barrier to engaging with clinical content.
I approached this as a global UX architecture problem with local experience design sensitivity requirements — defining first where structural consistency was non-negotiable, and identifying where local design variation was required. The IA and UX principles that had to hold across all markets were established centrally; specific flex zones where local teams needed full adaptive experience design control were explicitly named and designed for adaptation.
AI-assisted research and competitive analysis helped surface UX patterns and regional content gaps at scale across four markets. The Quiz Module was the highest-complexity local flex zone — a five-screen interactive questionnaire generating a personalized discussion guide, with significant variation requirements across markets.
Full UX and SEO audit of branded platforms (Wegovy.com, Qsymia.com, MyAlli.com) and Novo Nordisk's unbranded obesity platforms (ItsBiggerThan.com, TruthAboutWeight.global). Audit structured around Andrea's five content pillars: Empathize & Validate Patient Experience / Obesity Not Patient's Fault / Improve Health with Weight Loss / Tangible Solution — Address Biological Cause / Encouragement to Speak with HCP. Per-market search behavior analysis mapping colloquial vs. medical terminology in KSA (السمنة vs البدانة), Germany (Adipositas vs. Fettleibigkeit, 40K searches/month), and Japan (肥満, with notable stigmatizing language in search queries).
ItsBiggerThan.com (emotional/community) addressed empathy and health stakes but missed biological causation and HCP pathway. TruthAboutWeight.global (practical/scientific) addressed "not your fault" framing and biological cause but was weak on emotional validation and HCP conversion. Wegovy.com had 84% bounce rate despite 970K monthly visits — high traffic, low engagement. No competitor balanced all five pillars. Stigma was universal across all four markets, but manifested differently: social shame in Japan (searches included stigmatizing language), religious self-judgment in KSA/UAE, personal discipline failure framing in Germany.
Novo Nordisk owned the emotional stigma narrative. The white space was a platform that combined emotional validation with a practical action pathway — empathy first, biological framing second, treatment options third, social proof fourth, HCP conversation fifth. Four stigma-reduction modules as global constants. BMI calculator as a high-engagement SEO tool (TruthAboutWeight's 5.15 pages/visit came primarily from BMI search traffic). Market-specific terminology in flex zones.
Global wellness platforms & stigma-adjacent health conditions. The global constants / local flex zones architecture applies to any health platform scaling across markets where a condition carries cultural stigma. The stigma-reduction sequencing transfers directly to weight management, mental health, addiction support, and any condition where self-blame is a barrier to engaging with clinical content.
This site map framework defines the page hierarchy, content groupings, and experience design principles that had to remain consistent across all markets. The homepage anchored the experience with four stigma-reduction UX content modules before routing patients into four distinct experience pathways.
The site map established which UX elements were non-negotiable globally, giving regional teams a clear brief rather than an open brief — reducing late-stage drift across all four markets.
Four homepage modules forming the global constant zone — behaviorally sequenced to resolve shame, attribution, stakes, and agency before any clinical content is surfaced. Select a module to expand the design rationale.
Creates an opening without assigning blame. The patient must feel addressed, not judged, before any information has value.
The emotional barrier it resolves — shame-avoidance — is culturally invariant. Localising this module risks softening the activation signal.
Patient has accepted the premise that change is possible. Attribution of cause is still unresolved — must be addressed next.
Sequence constraint: modules must appear in this order across all market builds. Each resolves one emotional barrier before the next is surfaced. Reordering collapses the behavioral arc. Flex zones begin at section two of the site IA.
Five-section readiness ladder — each section has a gate condition that must be met before the next section's content has behavioral value. Select a section to expand content logic and global/flex designation.
Homepage — emotional foundation
Permission for the patient to engage with the subject at all. Shame and self-blame are resolved before any clinical information is presented.
The four stigma-reduction modules in fixed sequence. CTA is soft — discovery, not conversion. No clinical content until the module arc completes.
Understanding obesity — condition education
Clinical understanding of obesity as a chronic disease. Patient must accept the medical framing before treatment options carry credibility.
Global core: biology, comorbidities, systemic impact. Flex: specific comorbidity emphasis may be localised to market-prevalent conditions.
Weight management options — treatment landscape
Patient sees treatment as a legitimate, multi-modal space. HCP guidance is positioned as necessary context, not gatekeeping.
Global core: treatment categories and the role of medical management. Heavy flex: specific options, regulatory references, and reimbursement context vary by market.
Weight loss journeys — social proof layer
Patient confidence that people like them have navigated this. Social proof functions as risk-reduction — lowers perceived barrier to initiating an HCP conversation.
High flex zone. Patient stories reflect market demographics and locally prevalent emotional barriers. Voice and tone flex permitted.
Talk to your doctor — action conversion
Concrete action. Patient arrives having resolved shame, accepted the condition, mapped options, and seen social proof. The CTA is now a low-friction next step, not a leap.
Core: HCP conversation framing and preparation tools. Flex: HCP-finding tools, system entry points, and CTA phrasing vary by market access model.
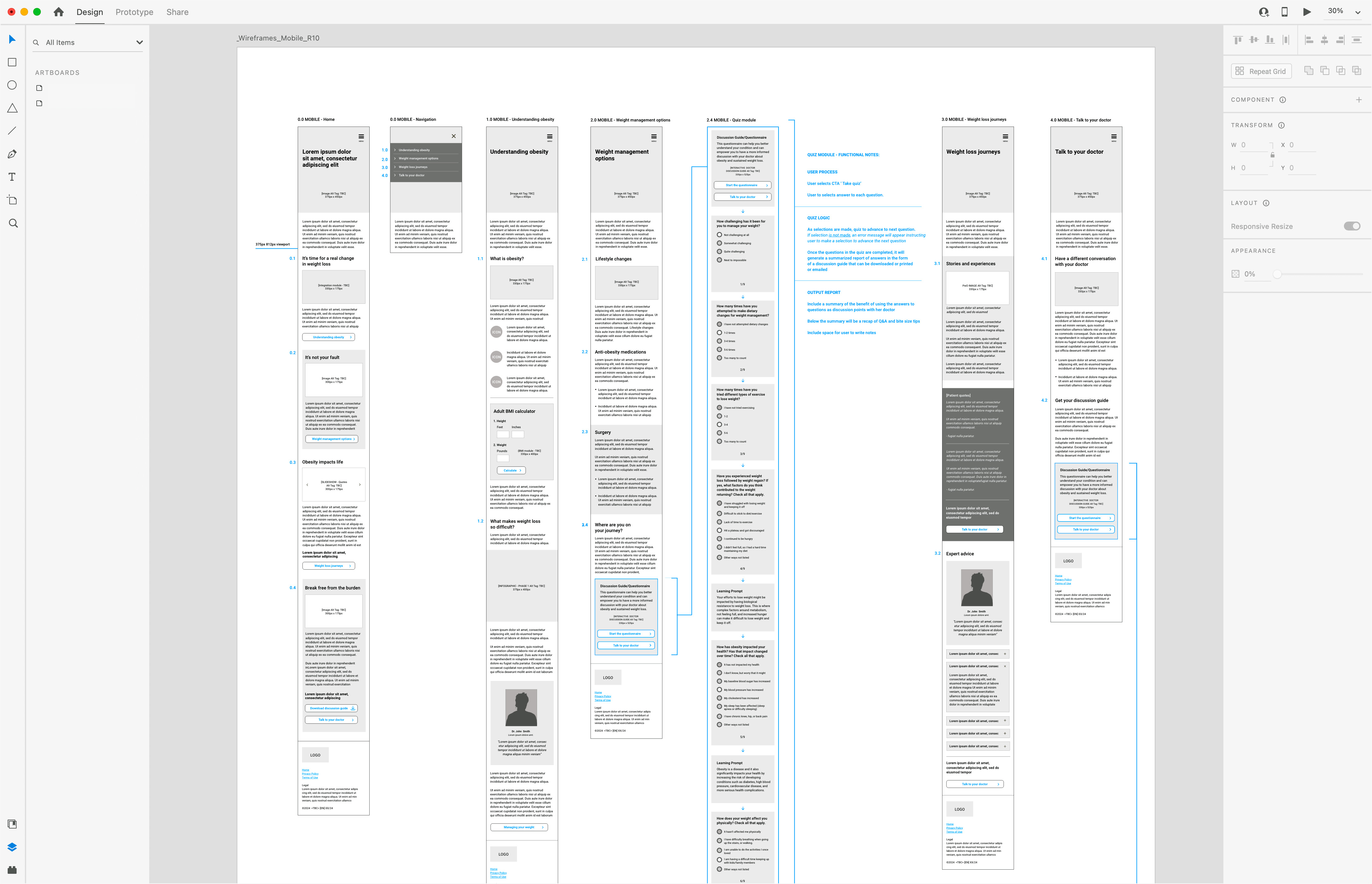
Mobile wireframes R10 — six-artboard mid-fidelity spread showing the complete five-section patient journey at 375px. Sections in sequence: Homepage (stigma-reduction module stack), Navigation, Understanding Obesity (condition education and BMI calculator), Weight Management Options, Quiz Module (personalized discussion guide generator), Weight Loss Journeys, and Talk to Your Doctor. The Quiz Module artboard documents functional logic across 9 questions with embedded learning prompts — clinical reframing delivered mid-flow at the moment a patient selects answers that signal biological resistance (e.g., "I continued to be hungry," "I didn't feel full") rather than deferred to the end of the questionnaire. The personalized output is downloadable as a PDF discussion guide for HCP conversations. All copy shown as lorem placeholder; structural hierarchy, interaction design, and UX sequencing are the deliverable. Pre-MLR working copy.
Seven validated mobile layouts gave regional teams reference implementations to adapt, not blank canvases — cutting per-market design time without sacrificing local precision.
Biological resistance cycle visualization — four design iterations (A, B, C1, C2) developed to make the self-reinforcing mechanism of obesity legible to Andrea without clinical language. The final format illustrates the cycle: lose a few pounds → increased hunger + change in metabolism + not feeling full → gain the weight back. MLR-viable because it shows mechanism without making a treatment claim. The design challenge was representing three simultaneous biological drivers (hunger, metabolism, satiety) acting on a single repeated outcome — a structural problem that required four rounds of design exploration to resolve cleanly across both desktop and mobile viewports.
MLR-approved global platform demonstrating that the stigma-reduction sequencing held across regulatory environments — used as the architecture proof for regional team briefings.
Global-to-local content architecture audit — competitive analysis benchmarking Novo Nordisk's content architecture across the emotional/practical axis in all four markets, classifying each dimension as globally fixed, locally adaptive, or a gap requiring local input before deployment.
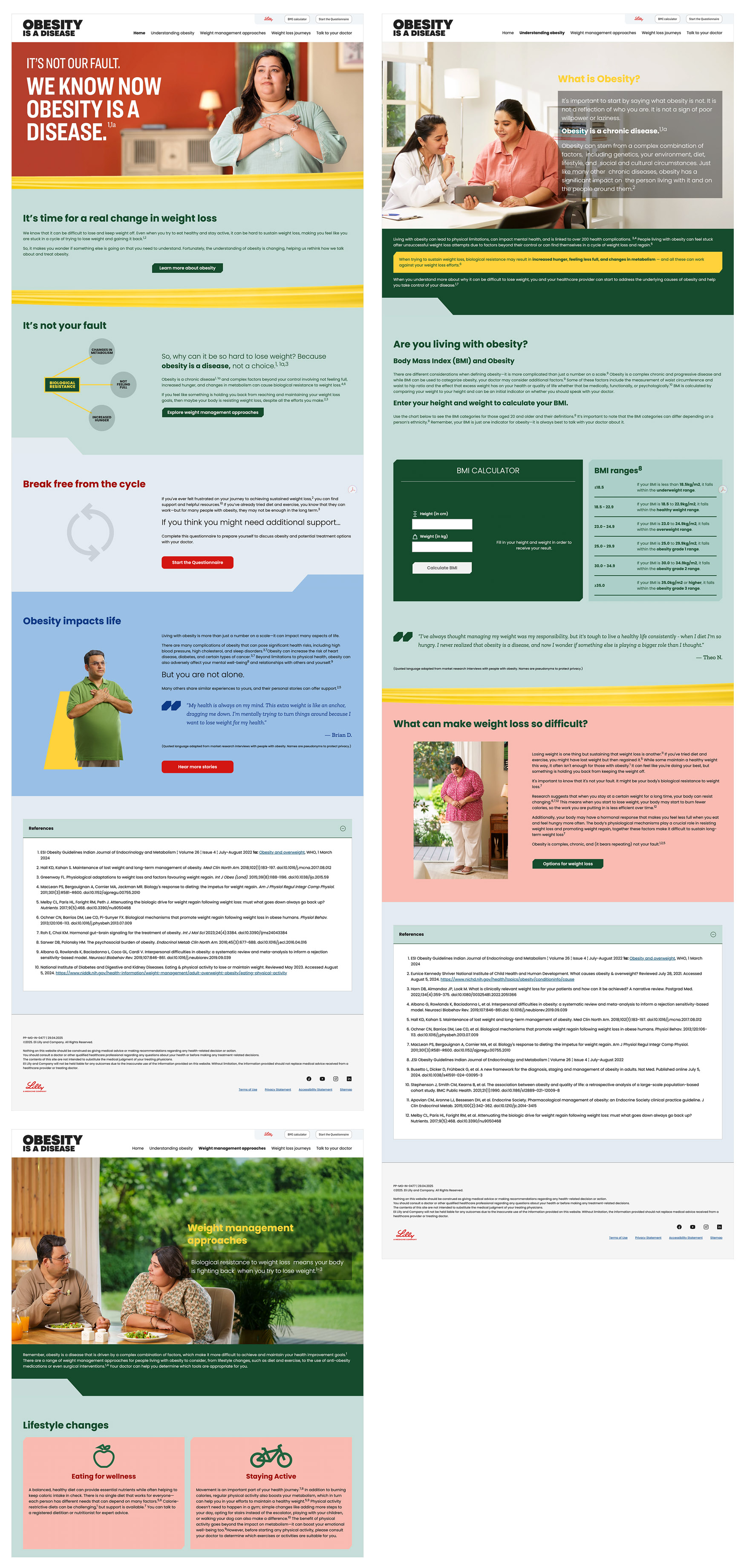
This is the fully produced global obesity platform submitted for MLR, with visual design carrying the stigma-reduction strategy as much as the copy does: a warm, editorial palette and full-bleed patient photography replacing the clinical iconography typical of the category. Homepage experience design opened with direct stigma-reduction framing ("The body can resist weight loss") before moving into the biological resistance UX flow. The Understanding Obesity page led with disease definition before introducing biological complexity through a carefully sequenced experience design hierarchy. The BMI calculator — surfaced as a high-engagement SEO tool based on competitive analysis showing TruthAboutWeight.global's 5.15 pages/visit driven by BMI search traffic — was embedded in the Understanding Obesity section.
The global/flex zone architecture scaled well across four markets. Local teams still needed a clearer signal — a governance decision tree telling them whether they're in a flex zone or a global constant, rather than catching drift in late-stage review. I'd also bring the AI research layer into cultural-sensitivity analysis earlier in the process. We applied it primarily to competitive pattern analysis; pointing it at regional patient voice content and health literacy signals during the research phase would have made the local flex zone design substantially more precise.